Feb 5, 2021 | Digital Dermatopathology, Digital Pathology
Images shown are not intended to be used for the diagnosis or treatment of a disease or condition.
Often mistaken clinically for a more common skin growth like an epidermoid cyst, pilomatricoma is the focus of this Digital Dermatopathology Digest episode with Rajni Mandal, MD.
Pilomatricoma is a benign skin growth that typically occurs in children and young adults. Studies show that around 40 percent of cases happen to patients under age 10, and 60 percent of cases appear before age 20. Interestingly, research also shows girls are about 50 percent more likely to develop a pilomatricoma than boys.
This growth is associated with the somatic mutation of CTNNB1 in the hair matrix cell, which leads to increased beta-catenin (decreased cell adhesion) and uncontrolled cell division through the Wnt signaling pathway.
Pilomatricomas have very distinguishing pathologic features. “The keratin within the center of pilomatricoma is quite characteristic,” explains Mandal. “You can see multiple holes, or ghosts, of the keratinocyte nuclei.”
Although pilomatricomas aren’t painful or malignant in nature, they don’t resolve on their own. Dermatologists may recommend a skin biopsy to rule out cancer—and because they continue to grow and often appear on the head and neck, most patients opt to have them removed.
To learn more about pilomatricoma and other skin conditions, click here for more episodes of PathologyWatch’s Digital Dermatopathology Digest.
Jan 29, 2021 | Digital Pathology, Uncategorized
Running a promising dermatology clinic means continuously seeking ways to enhance patient care quality and maximize staff efficiency. For proof, consider that over 40 percent of practices claim to have implemented EMR systems to help them grow.
While implementing an EMR system for dermatologists has many advantages, there are still some disadvantages to consider. This article will look at the pros and cons of electronic medical record systems for dermatologists, including reducing paper, image management, billing, lab interaction, and EMR limitations to ensure you have the facts when considering ways to maintain quality diagnosis and patient care.
Reducing Paper
One main advantage to an EMR is the ability to access your notes and patient information anywhere. In an increasingly digital world, we are often communicating with patients while out of the office. Still, 25 percent of dermatologists continue to use traditional paper systems to support their operations.
Here are some of the standard paper shortcomings and the ways an EMR system solves them:
- Repetitive tasks: Completing the same functions repeatedly takes time and energy away from vital patient interaction. In addition to autopopulating fields, an EMR sends data electronically, so it doesn’t have to be re-entered.
- Errors: Entering and re-entering data into the LIS introduces the possibility of human error. Entering data one time using an EMR removes the chance of making mistakes on repeat entries.
- Access: Pulling a patient’s paper file can only be done in the office, requiring time and physical space to store the physical records. Using electronic medical records means patient information is stored securely in the Cloud, which providers can instantly access from anywhere with a Wi-Fi connection.
Unlike paper, EMR systems make it increasingly advantageous for dermatologists and their staff to do things more efficiently and conveniently. It is important to ensure staff is adequately trained on a new system and receives regular review sessions to maintain a good standard of EMR charting, as updates occur several times per year.
Managing Images
Patient images in dermatology are valuable, as much of the specialty relies on visual recognition. It is also important when tracking the correct site of a biopsy, especially for referring to other providers like Mohs surgeons.
Digital images are easy to capture, but often cumbersome to organize. If not using an EMR, these will have to be organized in folders with patient name and date and kept in a secure digital environment. Many EMRs resolve this arduous process by allowing you to take photos within the patient chart and automatically assigns the images to the correct biopsy location. These images can be accessed immediately, making it easier for dermatologists to share them with partners and patients or review them on the next visit. Also, being able to review them in the context of your visit with relevant labs and other notes helps in diagnosis, especially of difficult cases.
Reliable Billing
While necessary, billing is not the favorite activity of most providers. However, billing takes time and diligence to communicate with insurance companies and resubmit claims when appropriate. With that in mind, another benefit of electronic medical records is the autobilling feature.
Many EMRs will issue invoices based on coding applications. In addition, some EMR systems claim up to 98 percent first-pass claim acceptance, which means you and your staff can spend time focusing on patient care instead of going back and forth with insurance companies.
Also, EMRs automatically track any changes to Medicare’s Merit-Based Incentive Payment System (MIPS), ensuring your practice receives accurate reimbursement for qualifying services. This eliminates manual tracking and helps you to maintain focus on patient care.
Lab Interaction
Communication with your dermatopathology lab partner is vital to ensure the highest quality of diagnosis for your patients. Full-service dermatopathology labs like PathologyWatch will integrate an EMR interface, which allows them to access the data and fields entered into your EMR system.
Equally important, an EMR interface grants you instant lab results and images sent directly to your device. The EMR also helps you send e-faxes to providers or drop notes directly to the patient’s record, instead of requiring your staff to print out, fax, scan, and wait for a confirmation.
EMR Limitations
While EMR systems embed many time-saving and workflow advantages, they also contain quirks and constraints that users learn to navigate. For instance, 82 percent of physicians indicate it takes too long to enter data that isn’t directly related to patient care.
The EMR could also make it difficult to communicate outside of the prescribed default descriptions. Thus, if you indicate eczema when you’re trying to describe a rash, it may take you longer to type in a custom description than selecting the available options. To make the system work right, you have to be willing to customize your process with templates, adding quick text or macros when possible to aid in customizing each note, and take time to delete unused or irrelevant items within your templates.
Sometimes, adding digital elements can create slow-downs if the interface is down or you experience an error after an update, for instance. This can be challenging if you can’t print out a requisition from your EMR or can’t access patient records while you are seeing patients in the clinic.
In the end, the benefits of implementing an EMR into your dermatology practice often outweigh the disadvantages. By understanding how EMR systems can reduce your reliance on paper, manage images, increase billing efficiency, and boost lab communication, your clinic can make a qualified decision that can help you continue to provide quality care for your patients.
Jan 21, 2021 | Digital Pathology
Images shown are not intended to be used for the diagnosis or treatment of a disease or condition.
In order to diagnose pathologic skin conditions, it’s important to first be able to recognize what constitutes normal skin and variants. In this Digital Dermatopathology Digest episode, Rajni Mandal, MD, uses a digital pathology image viewer to offer a quick summary of key characteristics in normal skin. Here are some video highlights.
Skin Anatomy
The body’s largest organ takes on a variety of appearances depending on the anatomic location. The two outermost layers—the epidermis and the dermis—work closely together. The epidermis, or outer layer, typically has four or five distinct layers of cells but lacks blood vessels or nerve endings.
The inner layer, or the dermis, consists of pink collagen fibers, which are connective tissue that supports, nourishes, and strengthens the epidermis. Also contained within the dermis are key structures such as nerve endings, blood vessels, lymph glands, hair follicles, and sweat glands.
“The dermis can vary in thickness based on location,” says Mandal. Skin of the back and trunk shows more compact collagen fibers and a thicker dermis compared to facial skin. Acral skin shows compact hyperkeratosis of the stratum corneum. Solar elastosis, seen in areas of sun damage, has a gray-purple hazy color and is a collection of excess elastic fibers.
Distinguishing Features of Adnexal Structures
Sebaceous glands have foamy cytoplasm and often attach directly to the hair follicle.
Deeper in the dermis, you can find eccrine sweat glands, which occur over most of your body and open directly onto the surface of your skin. “Eccrine ducts have a two-layer epithelium versus the eccrine glands, which have a single layer epithelium,” explains Mandal. Adipocytes are also found admixed around the glands.
By contrast, apocrine sweat glands are found in the axilla, nipple, ear canal, eyelid, scalp, and genital areas. Very round nuclei, eosinophilic cytoplasm, and eosinophilic secretions within the lumen are clues to apocrine glands.
If you enjoyed this summary of identifying normal skin and variants, or if you are preparing for boards and want to test your dermatopathology skills, check out this and other Digital Dermatopathology Digest instructional videos here.
Jan 11, 2021 | Digital Pathology, Pathology Business
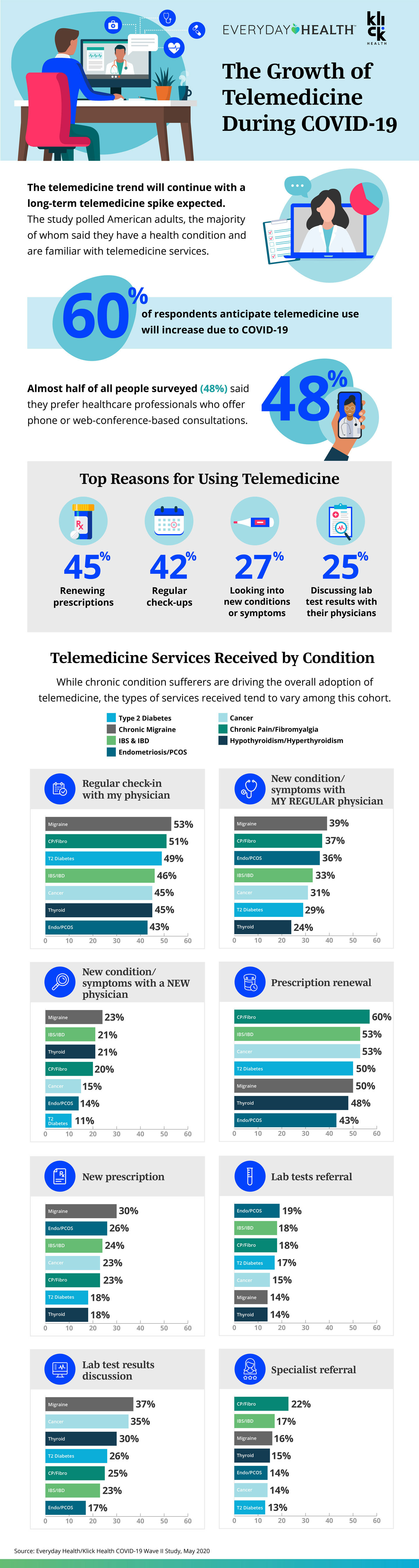
Despite the benefits touted by telemedicine enthusiasts, widespread adoption of this technology has lagged in the healthcare industry. However, with the onset of COVID-19, a new era of telemedicine has begun. Almost overnight, telemedicine became more accepted by regulators, providers, insurance companies, and patients. The combination of improved video technology, patient demand, and provider acceptance has eased restrictions and pushed telemedicine to the forefront in the medical industry.
In addition, dermatopathology is following this trend. Regulations for the remote use of pathology have changed in light of COVID-19, making it possible for pathologists to work remotely and support the use of digital pathology technology for the duration of the pandemic.
With the universal adoption of video conferencing, 20 percent of all medical visits are happening via telemedicine. Here are a few reasons to consider teledermatology:
Convenience
Recent surveys show that a common reason over one-third of patients may prefer telemedicine visits is saving time by avoiding the commute to a provider’s office. For instance, telemedicine can reduce the amount of time away from work or the cost and headaches of arranging childcare. Patients can be productive while waiting for the video conference instead of spending time in the waiting room. Even older patients who might have struggled with technology adoption in the past are more likely to embrace telemedicine options to avoid the increased COVID complications and mortality associated with this at-risk population.
Accessibility
Dermatologists can now use traditional billing codes for teledermatology visits. Teledermatology is accessible even when providers or patients may be out sick but are not debilitated. Many people who test positive for COVID are asymptomatic and would still like to keep their appointments if possible. This helps control the inevitable cancellations required for patients with cold symptoms and need to rule out COVID or flu infection before presenting in your office.
Because of increased access provided by digital dermatopathology, companies like PathologyWatch can employ a national network of dermatopathology experts. Many areas do not have access to dermatopathologists and often rely on expensive locum tenens to provide specialty or overflow care. Also, it can take several weeks to get a second opinion on a case. With a digital workflow, digital slides can be more quickly accessed for consensus diagnosis or consultation.
Teledermatology also provides people living in rural areas or mobility challenges with easy access to medical care using synchronous live video-conferencing. The CDC indicates that telemedicine “can help reduce barriers to care for people who live far away from specialists or who have transportation or mobility issues.” As one dermatologist described, “Our specialty is a visual field, and there are many skin conditions which are diagnosable from looks alone.” Dermatology lends itself well to photographic consultations by primary care providers to dermatologists.
Safety
During the COVID pandemic, the CDC established guidelines to keep healthcare workers and vulnerable patients safe during face-to-face visits. Despite these precautions, healthcare workers are still seven times more likely to develop severe COVID-19 infection than individuals performing nonessential jobs.
Teledermatology encourages a workflow that keeps providers and their staff safe from contracting diseases from patients or other staff members. Also, video conferencing can allow for the outsourcing of specific tasks, such as a scribe. This can help dermatology clinics by having a safe pool of healthcare workers that don’t have a higher risk of developing COVID-19.
Patient Satisfaction
Up to 48 percent of people prefer providers who offer telemedicine visits. A consumer survey revealed that 75 percent of patients who participated in virtual care were very or completely satisfied with the experience.
Meanwhile, telemedicine can level the socioeconomic playing field. Access Derm is an AAD-supported teledermatology program where volunteer dermatologists can help underserved populations who don’t have access to a dermatologist. It helps provide critical preventive care and second opinions, improving the quality of life and reducing the expense of future treatments by diagnosing skin cancer at earlier stages, for example.
When to Consider Teledermatology
Consider teledermatology options for follow-up visits that focus primarily on counseling rather than diagnosis. With these types of patients, rapport has already been established through in-person visits, and with straightforward diagnoses—like acne, atopic dermatitis, and psoriasis—much of the return visit focuses on review of lab work, medication counseling, and treatment changes if patients are not responding to first-line therapies. In particular, iPLEDGE patients or their caregivers, who are required to have monthly visits for the duration of therapy, may save significant time through a teledermatology visit.
While not all visits are possible through video conferencing, making healthcare convenient can encourage more people to seek regular consultations and take better care of themselves.
Dec 30, 2020 | Digital Pathology
Images shown are not intended to be used for the diagnosis or treatment of a disease or condition.
In this episode of Digital Dermatopathology Digest, Rajni Mandal, MD, a dermatopathologist at PathologyWatch, discusses the most common dermatological malignancy—basal cell carcinoma (BCC)—including how common it is, its warning signs, and characteristics of its various forms.
How Common Is BCC?
Prolonged exposure to UV sunlight or indoor tanning contributes to this and other forms of skin cancer, which triggers mutations in p53, PTCH (sonic hedgehog pathway), and SMO gene. Research shows that four million Americans are diagnosed with basal cell carcinoma every year. Most cases occur in people over the age of 50, and men are more likely to develop BCC than women.
What Are The Most Common Subtypes?
“There are two common types: nodular and superficial,” explains Rajni. She also points out the aggressive types of basal cell carcinoma include infiltrative, micronodular (which presents characteristics similar to those of the nodular subtype, except it’s comprised of multiple nodules), morpheaform, and basosquamous subtypes.
What Are Differences between Superficial and Nodular BCC?
Features of superficial BCC include clusters of basaloid cells descending from the epidermis with no dermal invasion.
The most common subtype, nodular basal cell carcinoma has islands of cells with peripheral palisading and a haphazard arrangement of the more central cells.
What Are the Characteristics of Morpheaform BCC?
Also known as sclerosing basal cell carcinoma, this aggressive subtype has spiky, basaloid, thin cell strands that chase down the dermis with its dense fibrous stroma. Differential diagnoses may include metastatic cancer, microcystic adnexal carcinoma, and desmoplastic trichoepithelioma.
What Are Clinical Symptoms of BCC?
Patients with basal cell carcinoma may experience:
- Sores that don’t heal
- Patches of skin that remain irritated and red
- A bump of skin that may resemble a mole but appears shiny, pink, or pearl-like in appearance
- An area where skin looks shiny and taut with poorly defined borders and a scar-like appearance
These symptoms are most likely to occur in areas often exposed to the sun, such as one’s face, neck, scalp, back, shoulders, ears, and chest. Other risk factors include Gorlin syndrome and nevus sebaceus.
Whether you’re in residency, studying for board exams, or a practicing dermatologist looking to stay sharp, the Digital Dermatopathology Digest video series is your informational and convenient source for dermatopathology review. Find the full series here.
Dec 18, 2020 | Digital Dermatopathology, Digital Pathology
Images shown are not intended to be used for the diagnosis or treatment of a disease or condition.
An epidermal inclusion cyst is the most common cutaneous cyst, often called a sebaceous cyst, which is actually a misnomer. The center of epidermoid cysts almost always contains keratin and not sebum. This keratin often has a “cheesy” appearance. They also do not originate from sebaceous glands; therefore, epidermal inclusion cysts are not truly sebaceous cysts.
In this episode of Digital Dermatopathology Digest, Rajni Mandal, MD, dermatopathologist at PathologyWatch, explains the common characteristics of an epidermal inclusion cyst.
“An epidermal inclusion cyst has an epidermis-like lining with a granular layer,” explains Mandal—as opposed to a nongranular layer, seen in a pilar cyst or steatocystoma. “Sometimes there is a connection with the overlying epidermis known as a punctum.”
Mandal goes on to mention features, the lack of which can help distinguish epidermal inclusion cysts from other common cysts, including dermoid, pilar, and vellus cysts.
Ruling Out a Dermoid Cyst
A dermoid cyst has cell walls that contain hair follicles, sweat glands, and other multiple adnexal skin structures. By contrast, an epidermal inclusion cyst lacks adnexal structures.
Ruling Out a Pilar Cyst
What makes a pilar cyst unique is that it arises from the epithelium between the sebaceous gland and the arrector pili muscle. They are lined by stratified squamous epithelium without a granular cell layer, similar to what is seen in the outer root sheath of the hair follicle, and filled with keratin.
Often presenting themselves as a round, dome-like bump, a pilar cyst is typically firm to the touch but not painful for the patient, while an epidermal inclusion cyst may become inflamed and painful to the touch.
Ruling Out a Vellus Hair Cyst
If small hairs appear in the vellum, with small red or brown bumps and a smooth dome shape, and often occur over the sternum, it is likely a vellus hair cyst.
Whether you’re in residency, studying for board exams, or a practicing dermatologist looking to stay sharp, the Digital Dermatopathology Digest video series is your informational and convenient source for dermatopathology review. Find the full series here.
{kind=link}